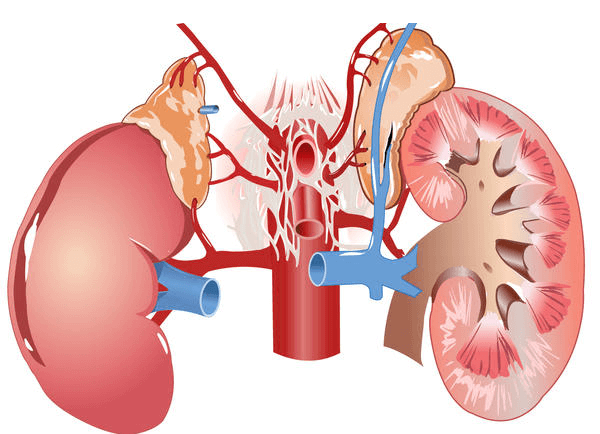
Our Kidney Failure which are also called the master chemist of the body maintains the electrolytic balance of the body fluid, maintains the osmolarity and acid – base balance.
1. The kidneys are the key organs to maintain the balance of the different electrolytes in the body and the acid-base balance. In case of Kidney failure progressive loss of kidney function results in a number of adaptive and compensatory Renal and Extra-renal changes that allow homeostasis to be maintained with Glomerular filtration rates in the range of 10-25 ml/min. With Glomerular filtration rates below 10 ml/min, there are almost always abnormalities in the body’s internal environment with clinical repercussions.
2. Water Balance Disorders: In advanced chronic Kidney Failure disease (CKD), the range of urine osmolarity progressively approaches plasma osmolarity and becomes isostenuric. This manifests clinically as symptoms of nocturia and polyuria, especially in tubulointerstitial kidney diseases. Water overload will result in hyponatremia and a decrease in water intake will lead to hypernatremia. Routine analyses of serum Na levels is performed in all patients with advanced CKD. Except in edematous states, a daily fluid intake of 1-1.5 liters should be recommended. Hyponatremia does not usually occur with Glomerular filtration rates above 10 ml/min. If it occurs, an excessive intake of free water should be considered or nonosmotic release of vasopressin by stimuli such as pain, anesthetics, hypoxemia or hypovolemia, or the use of diuretics. Hypernatremia is less frequent than hyponatremia in CKD.
3. Sodium Balance Disorders: In CKD, fractional excretion of sodium increases so that absolute sodium excretion is not modified until Glomerular filtration rates below 15 ml/min. Total body content of sodium is the main determinant of extracellular volume and therefore disturbances in sodium balance will lead to clinical situations of volume depletion or overload: Volume depletion due to renal sodium loss occurs in abrupt restrictions of salt intake in advanced CKD. It occurs more frequently in certain tubulointerstitial kidney diseases (salt losing nephropathies). Volume overload due to sodium retention can occur with Glomerular filtration rates below 25 ml/min and leads to edema, arterial hypertension and heart failure. The use of diuretics in volume overload in CKD is useful to force natriuresis. Weight and volume should be monitored regularly in the hospitalized patient with CKD.
4. Potassium Balance Disorders: In CKD, the ability of the kidneys to excrete potassium decreases proportionally to the loss of glomerular filtration. Stimulation of aldosterone and the increase in intestinal excretion of potassium are the main adaptive mechanisms to maintain potassium homeostasis until glomerular filtration rates of 10 ml/min. The main causes of hyperkalemia in CKD are the following: Use of drugs that alter the ability of the Kidney Failure to excrete potassium: ACEIs, ARBs, NSAIDs, aldosterone antagonists, nonselective beta-blockers, heparin, trimetoprim, calcineurin inhibitors. Determination of serum potassium two weeks after the initiation of treatment with ACEIs/ARBs is recommended. Routine use of aldosterone antagonists in advanced CKD is not recommended. A low-potassium diet is recommended with GFR less than 20 ml/min, or GFR less than 50 ml/min if drugs that raise serum potassium are taken. In the absence of symptoms or electrocardiographic abnormalities, review of medications, restriction of dietary potassium and use of oral ion exchange resins are usually sufficient therapeutic measures. Parenteral bicarbonate and ion exchange resins in enemas are not recommended as first-line treatment. Hemodialysis is considered in patients with glomerular filtration rates below 10 ml/min.
5. Acid-Base Disorders in CKD: Moderate metabolic acidosis (Bic 16-20) mEq/L is common with Glomerular filtration rates below 20 ml/min, and favors bone demineralization due to the release of calcium and phosphate from the bone, chronic hyperventilation, and muscular weakness and atrophy. Its treatment consists of administration of sodium bicarbonate, usually orally (0.5-1 mEq/kg/day), with the goal of achieving a serum bicarbonate level of 22-24 mmol/L. Limitation of daily protein intake to less than 1 g/kg/day is also useful. Use of sevelamer as a phosphate binder aggravates metabolic acidosis since it favors endogenous acid production and therefore acidosis should be monitored and corrected if it occurs. Hypocalcaemia should always be corrected before metabolic acidosis in CKD. Metabolic acidosis is an infrequent disorder and requires exogenous alkali administration (bicarbonate, phosphate binders) or vomiting.
Homeopathic Aspect
With the help of Homeopathic medicines acid base balance along with Osmolarity can be maintained. The electrolyte balance with symptoms can also be corrected with Homeopathic medicines, moreover the Homeopathic medicines if used in high dilutions (NANO Form) do not contain any crude drug material, hence are totally harmless with no side effects.